Sagittal Alignment of the Neutral Spine
The purpose of this page is to demonstrate the scientific support of the geometric configuration chosen for our 3D model of the spine. This alignment is also selected as the default spine position for the application "Biomechanics of the Spine."


The sagittal alignment of the spine describes the curvature of the spine in the sagittal plane. The key points of that description are the spine's physiological curves–cervical/lumbar lordosis and thoracic/sacral kyphosis. However, it is a simplified representation that could be compared to the iceberg size estimation by looking at its top part seen above the water. The more robust perception also includes the geometry and spatial orientation of the sacrum and pelvis, the global sagittal balance of an axial skeleton, and the projection of gravity centerline to the spine curves:
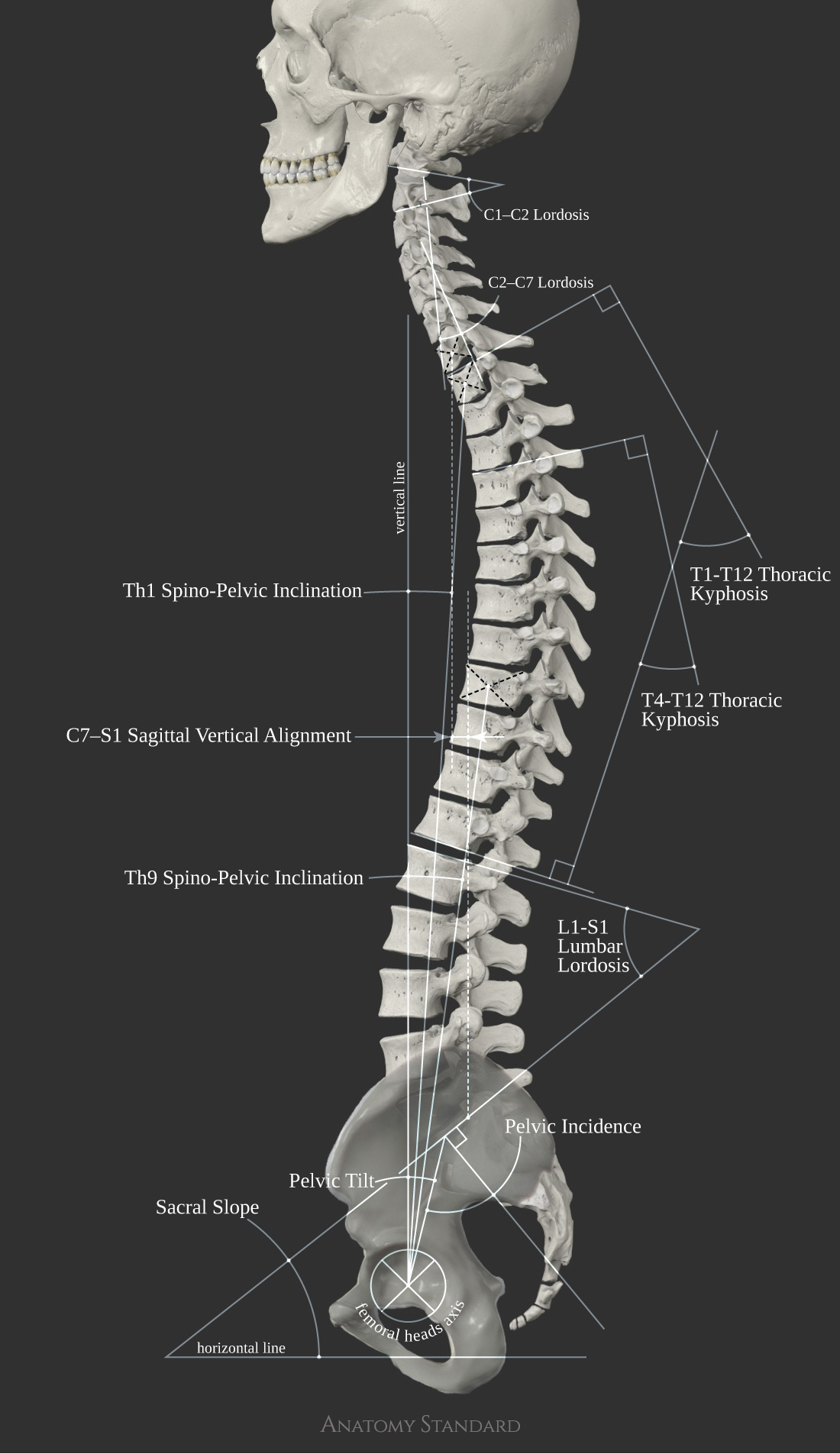

The set of measurements used to build the model of the human spine.
It is surprising, but there is no universal formula for the neutral sagittal alignment of the spine. Each angle and distance is with a relatively large variance. The best way to illustrate that phenomenon is to cite one of the most relevant sources–the textbook "Clinical biomechanics of the spine" by White and Panjabi–"The normal lumbar lordosis angle supported by the 20–40-year-old literature data lies within large range from 20° to 70° and an analogous thoracic kyphosis angle–from 20° to 50°".
Since these words were written, the medical imaging technique and methodology applied in research evolved significantly. Now we know more about multiple factors affecting the physiological curves of the spine, like differences between genders and ethnic groups (Roopnarian 2011, Zhu 2014), changes of spine curves during a lifetime (Iorio 2018), and an effect of physical activity (Todd 2015). However, even after selecting the study data by sex and age, we see highly variable results. This is why the choice of a particular configuration for our model was navigated by the range of standard deviations reported in multiple research papers and not by the data from the single trustable source.
The literature review presented in this webpage is in the form of graphs that were composed following the uniform logic:

The review is arranged in 3 parts. The first focuses on the spine's physiological curves (kyphoses and lordoses), the second part reviews the geometry and spatial orientation of the pelvis, and, finally, the third is dedicated to the global sagittal balance of the spine as a whole.
The Neutral Spine Curves for an Adult Man in Standing Standard Anatomical Position
The Cervical Lordosis
An evaluation of the cervical lordosis angle usually includes at least two levels: (1) angle between C1–C2 and (2) cervical lordosis from C2 to C7. The angle between C1–C2 in our model is equal to 23.5° that is in agreement with literature data.

The C1–C2 angle was subtended by a line drawn parallel to the inferior aspect of C1 and a line drawn parallel to the inferior endplate of C2
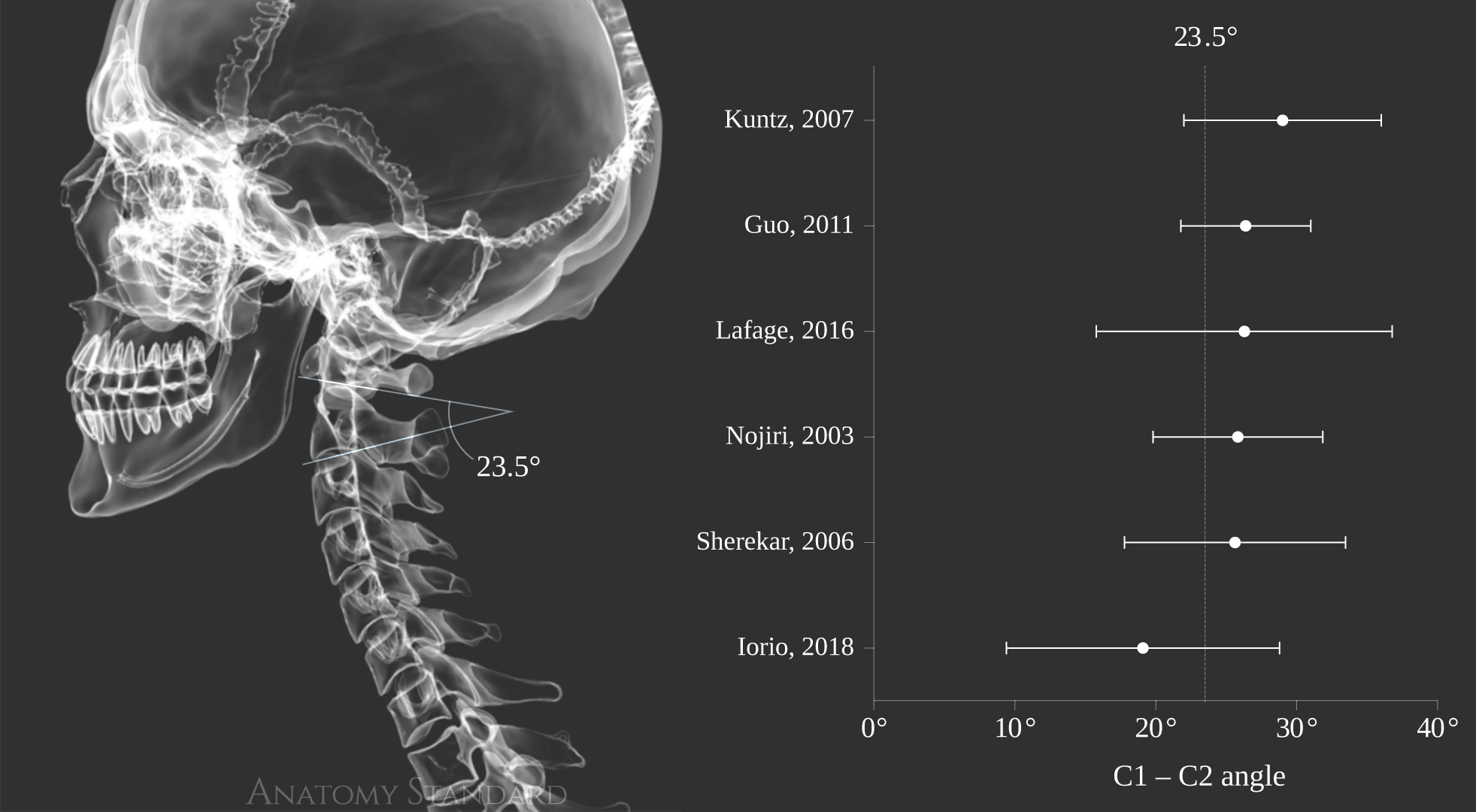

Scientific evidence for C1–C2 angle 23.5°
The cervical lordosis from C2 to C7 in our model is 17.7°, which is close to the average reported values in multiple studies. However, this cervical lordosis angle may be higher than reported for some Asian populations (Hasegawa 2017, Ao 2019).

The C2–C7 angle was subtended by a line drawn parallel to the posterior border of the C2 vertebral body and a line drawn parallel to the posterior border of the C7 vertebral body
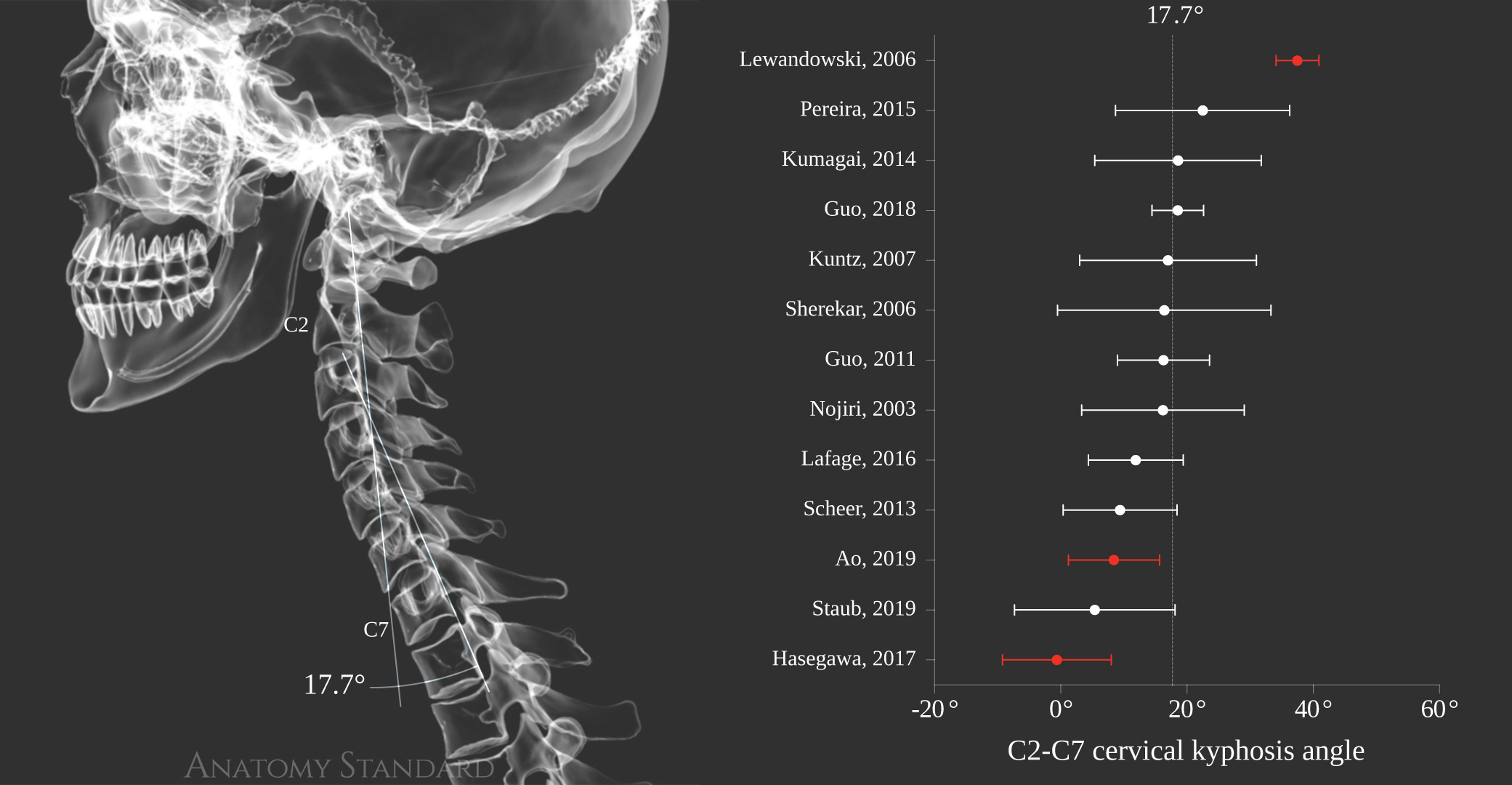

Scientific evidence for C2-C7 cervical kyphosis 17.7°
The Thoracic Kyphosis
The most commonly used methods for measuring thoracic kyphosis are (1) the angle between the Th1 upper plate and the Th12 lower plate or (2) the angle between the Th4 upper plate and Th12 lower plate. The corresponding kyphosis angles for our 3D model are respectively 30.7° and 47.0°. These angles fit well into the range reported in the scientific literature.

Thoracic kyphosis angle was measured from the superior endplate of Th1 and Th4 to the inferior endplate of Th12
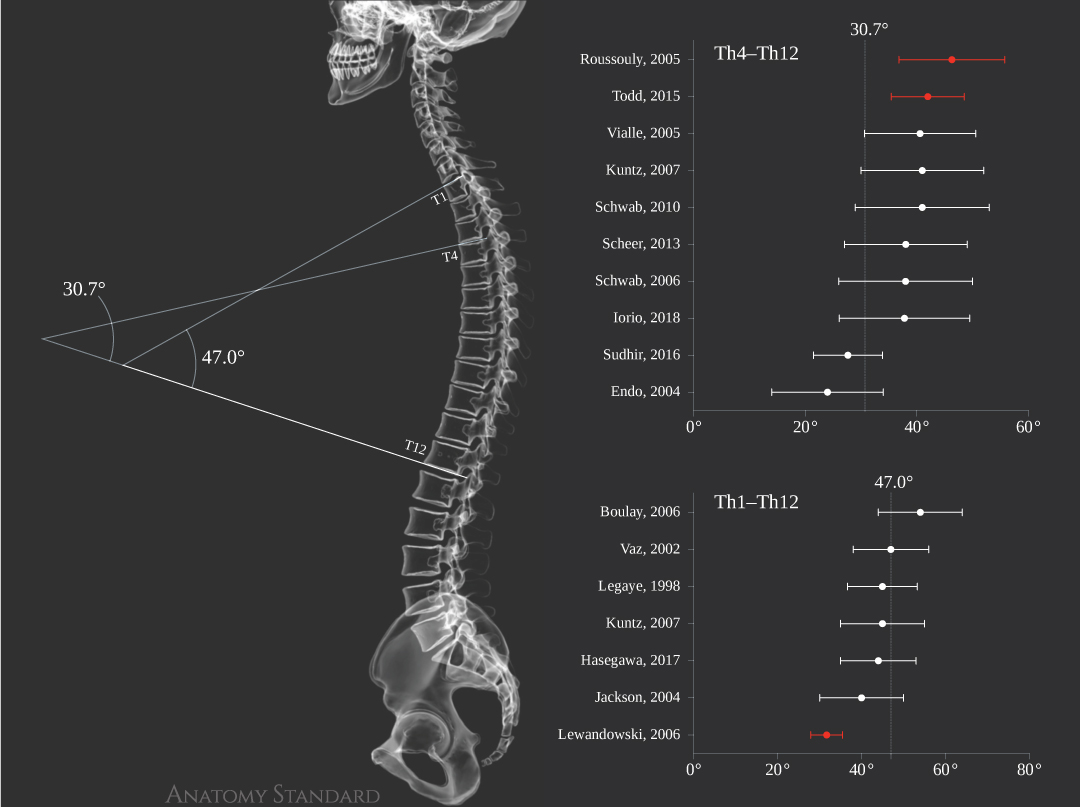

Scientific evidence for Th4–Th12 angle 30.7° and Th1–Th12 angle 47.0°
The Lumbar Lordosis
The lumbar lordosis measurement technique differs between the studies. Below we rely on the most commonly used approach – angle measurement from the L1 upper plate to the S1 upper plate. Our model lumbar lordosis is equal to 55.3° that fits within the range from 36°(Endo 2014) to 63.5°(Legaye 2008) reported in many recent studies.

Lumbar lordosis was measured from the superior endplate of L1 to the superior endplate of S1
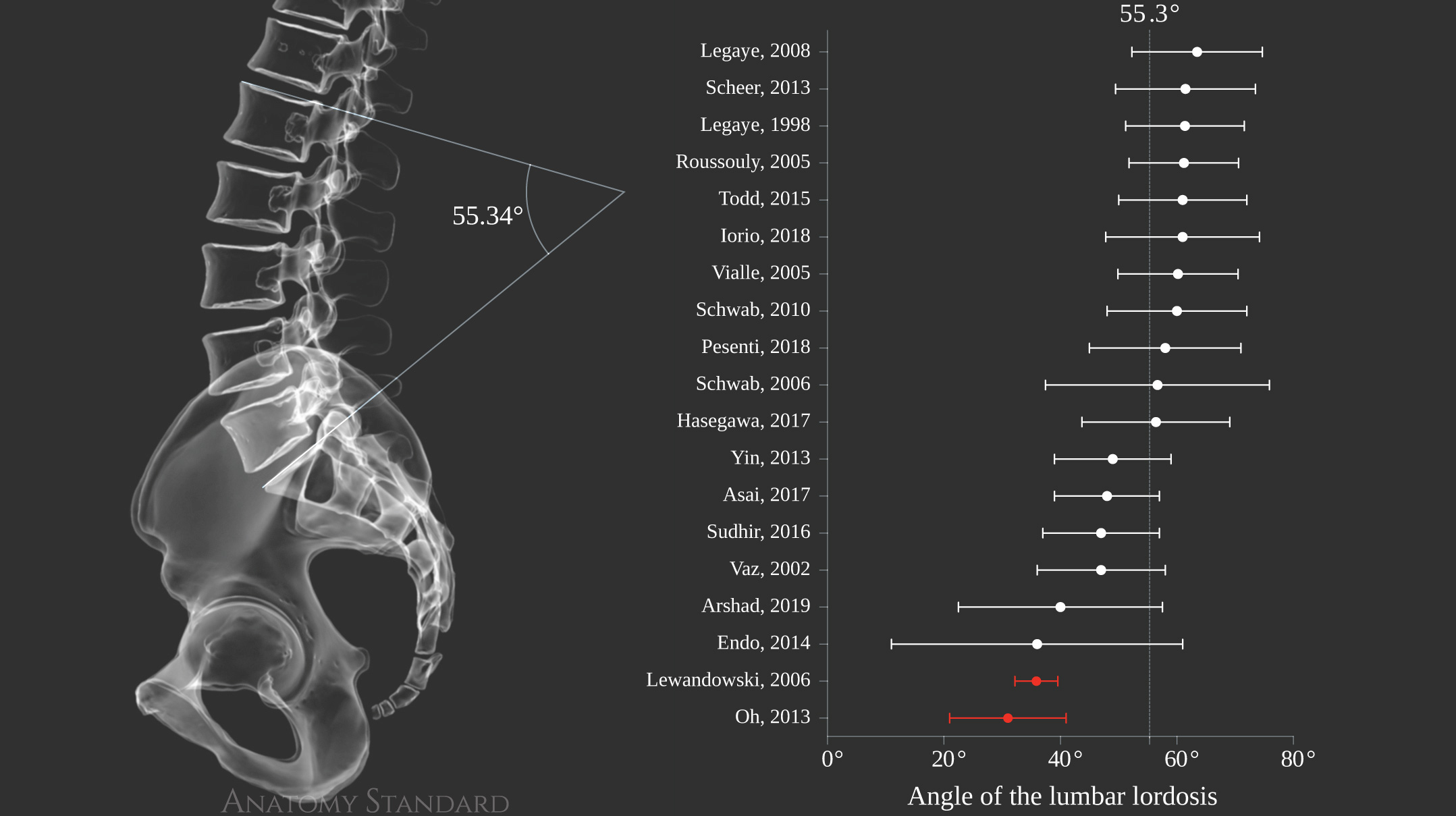

Scientific evidence for L1–S1 lumbar lordosis equal to 55.3°
The Configuration and Spacial Orientation of the Pelvis
The Sacral Slope
The sacral slope is considered one of the primary determinants of the lumbar spine curvature (Roussouly 2011b, Duval-Beaupère 1992) and the spine as a whole. The sacral slope of the Anatomy Standard spine model is 38.8° that is in agreement with the range generally accepted as a standard for a healthy spine and allocates the spine of our 3D model to Type 3 according to the classification proposed by Roussouly and colleagues in 2003 (Roussouly 2003). This type of spine curvature being reported as the most common for young and physically active men (Todd 2015).

The sacral slope was defined as the angle subtended by a horizontal reference line and the sacral endplate
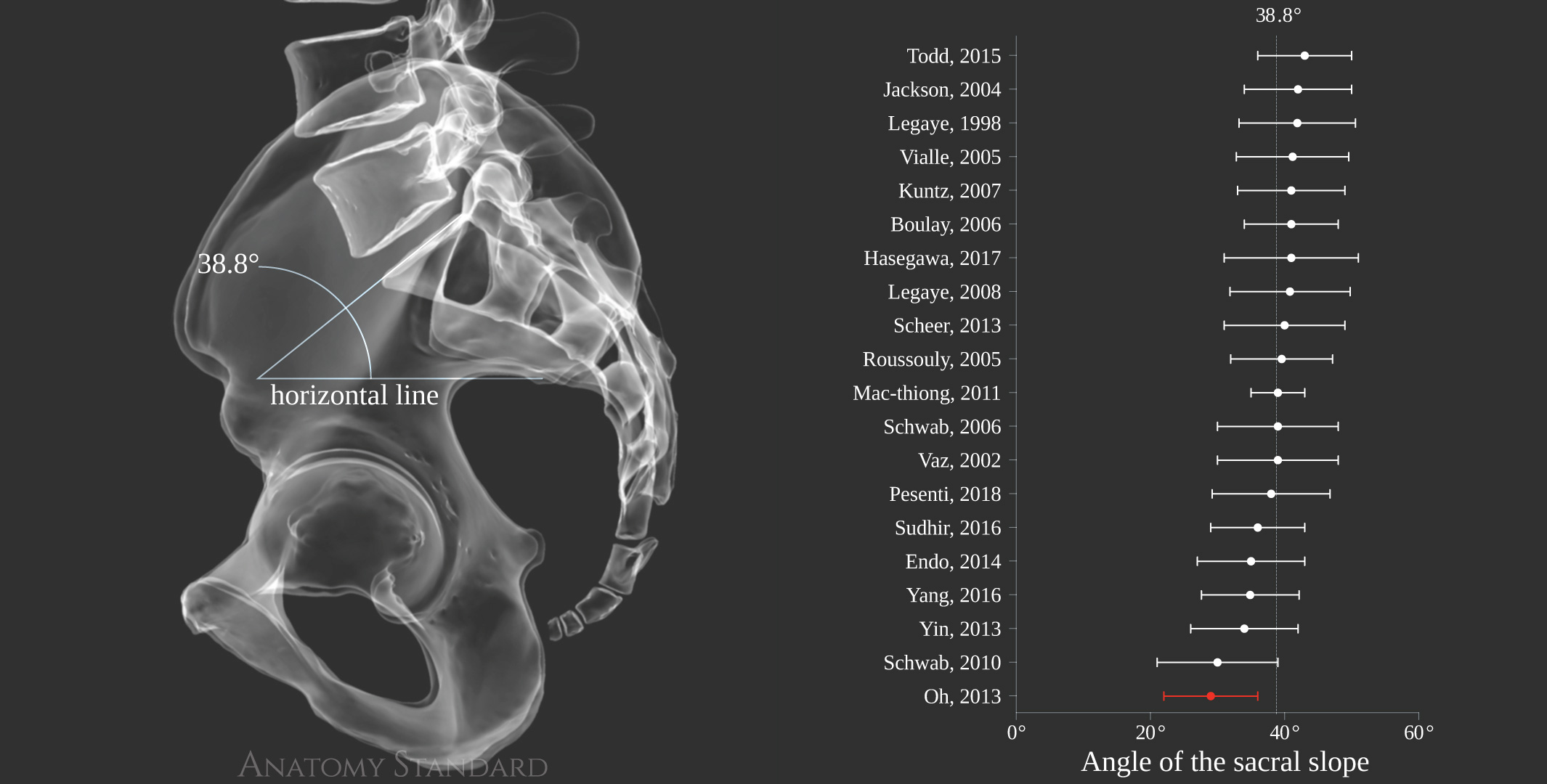

Scientific evidence for the sacral slope equal to 38.8°
The Pelvic Tilt
Pelvic tilt represents a pelvic rotation in the sagittal plane (Le Huec 2011) that now substituted pelvic inclination mentioned in older literature sources (Platzer 2003; Anda 1990). The pelvic tilt of our 3D model is 14.0°, and it is strongly evidence-based.

The pelvic tilt was defined as the angle subtended by a vertical line through the femoral heads axis and a line drawn from the midpoint of the sacral endplate to the femoral heads axis
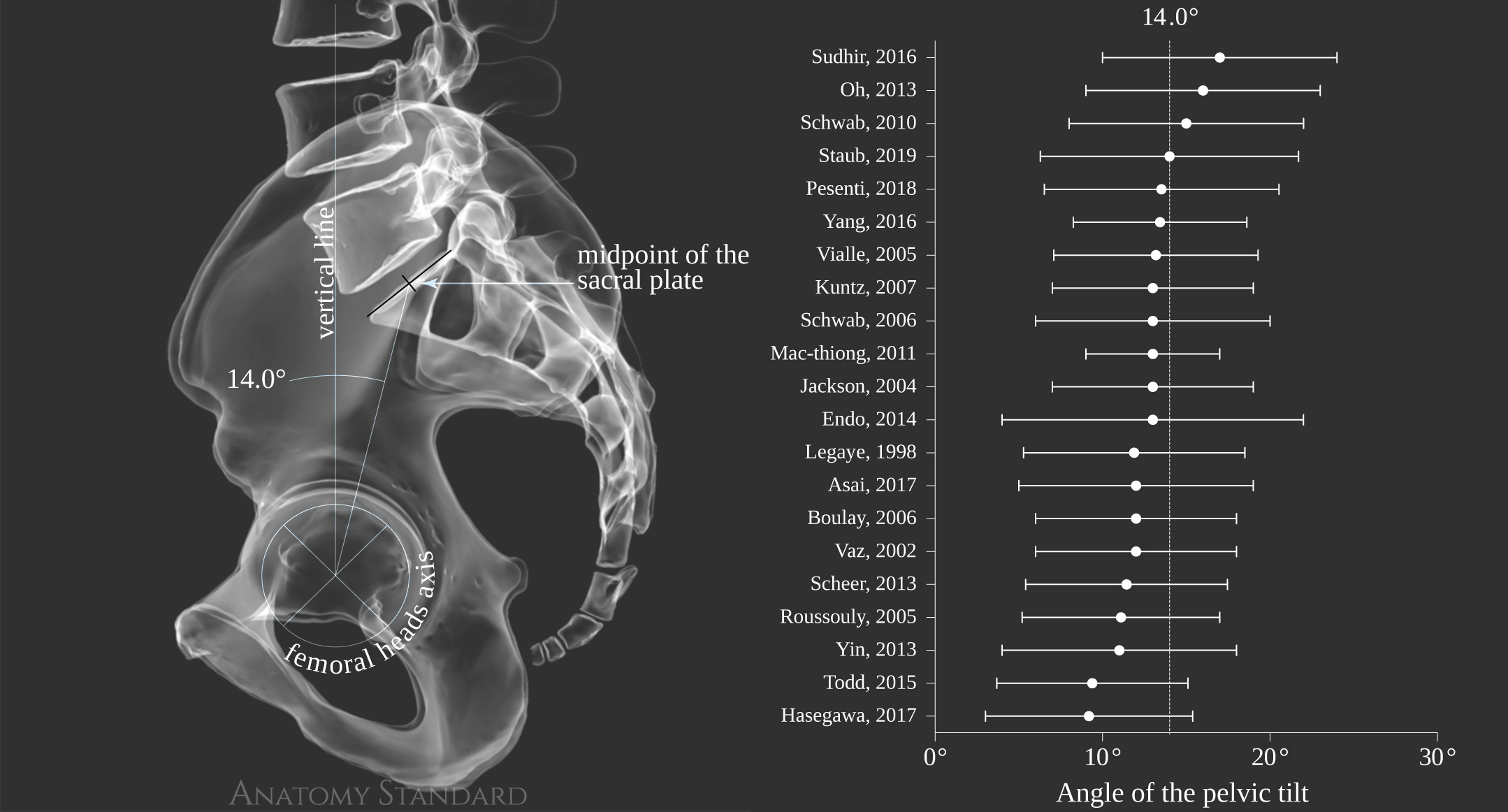

Scientific evidence for the pelvic tilt 14.0°
The Pelvic Incidence
The pelvic incidence is an integral parameter deriving from the sacral slope and pelvic tilt, affecting both the sagittal curvature of the spine and the pelvis's spatial orientation in a standing position. It is supposed to be a fundamental pelvic parameter for the spinal curves' three-dimensional regulation (Legaye 1998). Our model's pelvic incidence is 52.7° that agrees with the literature data.

The pelvic incidence was defined as an angle subtended by a line drawn from the femoral heads axis to the midpoint of the sacral endplate and a line perpendicular to the sacral endplate
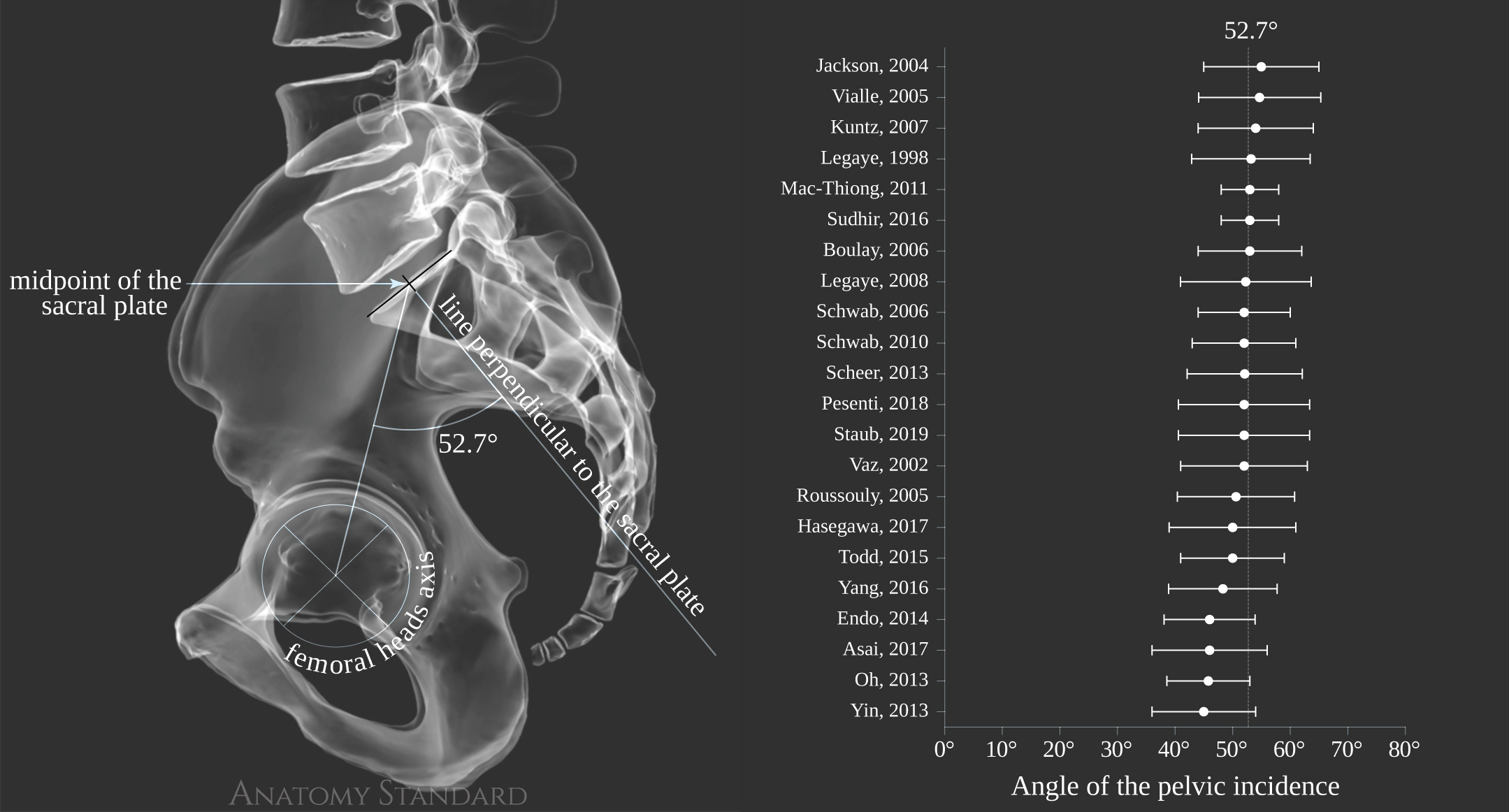

Scientific evidence for the pelvic incidence 52.7°
The Global Sagittal Balance of an Axial Skeleton
Many methods were proposed to assess the global sagittal balance of the spine, which is a strong predictor of the health-related quality of life in adults with spine deformities (Roussouly 2011a; Protopsaltis 2014; Mac-Thiong 2009). The most commonly reported are C7-S1 sagittal vertical alignment and Th1/Th9 spinopelvic inclination (Protopsaltis 2014; Legaye 2005).
C7–S1 Sagittal Vertical Alignment (SVA)
The C7-S1 SVA distance for our spine model is 10.0 mm that generally fits in the range of the data reported in the scientific literature for young men.

C7-S1 SVA is the horizontal distance from a vertical line centered to the C7 body to the posterosuperior corner of the S1 endplate
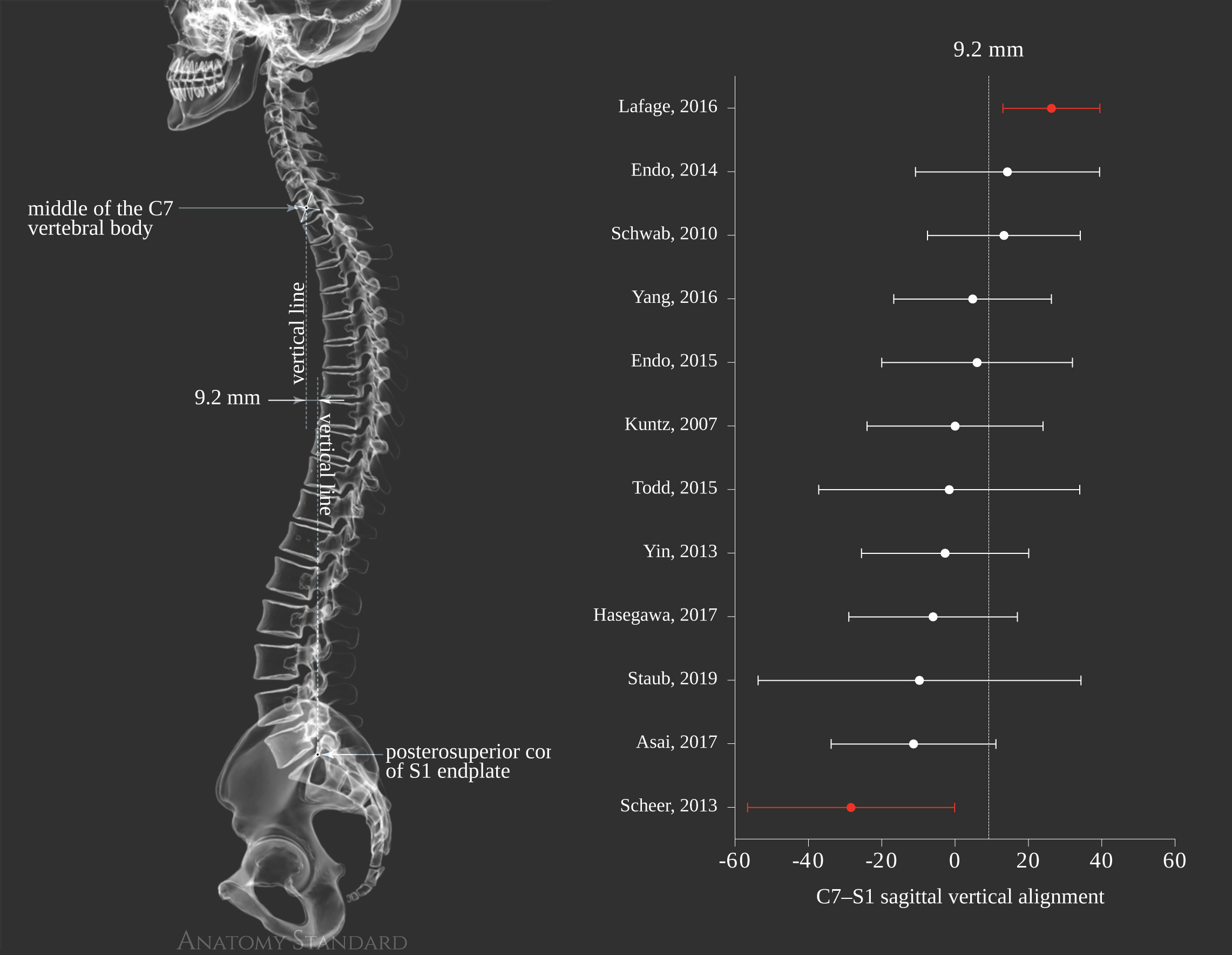

Scientific evidence for C7-S1 SVA equal to 9.2 mm
Th1 and Th9 Spinopelvic Inclination
Th1 and Th9 spinopelvic inclination reflect the global sagittal balance of the spine. The value of Th1 (3.5°) and Th9 (7.6°) spinopelvic inclination is within or very close to the standard deviation range reported in the literature.

Spinopelvic inclination angle was subtended by a vertical reference line through the femoral heads axis and a line drawn from the midpoint of the Th1 or Th9.
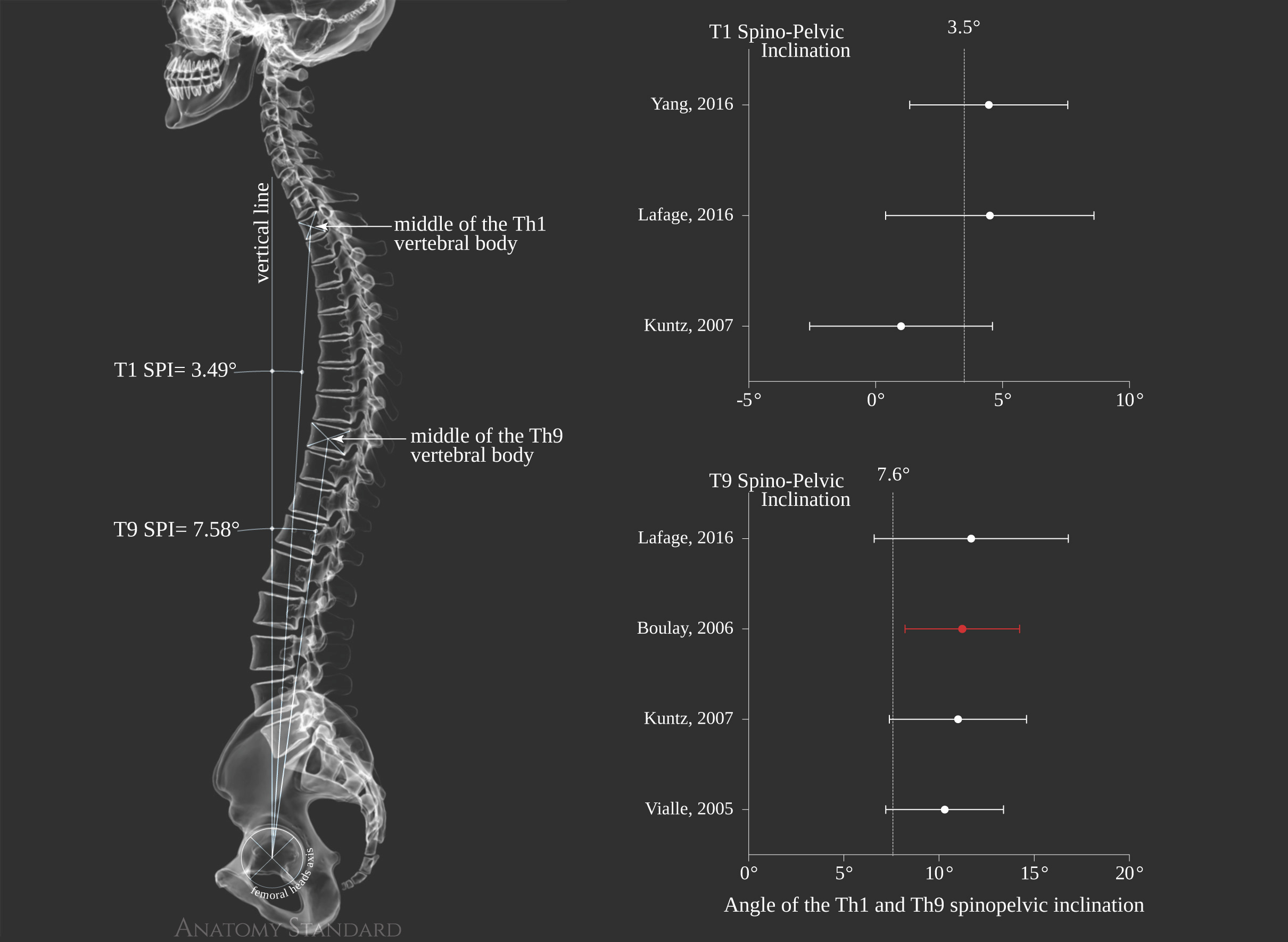

Scientific evidence for the Th1 spinopelvic inclination equal to 3.5° and the Th9 spinopelvic incedence equal to 7.6°
The Sagittal Projection of the Gravity Line to the Axial Skeleton
An equilibrium of the healthy human body in general and an axial skeleton specifically is closely related to the center of gravity or so-called gravity line. In recent decades a lot of evidence was accumulated about the projection of gravity line to the skeletal landmarks and the correlation of this projection with the aging process (Hasegawa 2017) and different pathological conditions (During 1985; Mac-Thiong 2009).
According to the barycentremetric studies, the gravity centerline of the well-balanced body with the kyphosis above 30° cross the body in front of Th9 ± 1.5 cm anterior to the vertebral body (Legaye 2008, Duval-Beaupère 1992). Caudally the projection of gravity center is 36.1 ± 20.6 cm behind the femoral head axis. Under such conditions, no muscular electric activity is observed in the posterior spinal muscles to maintain the body's vertical position.
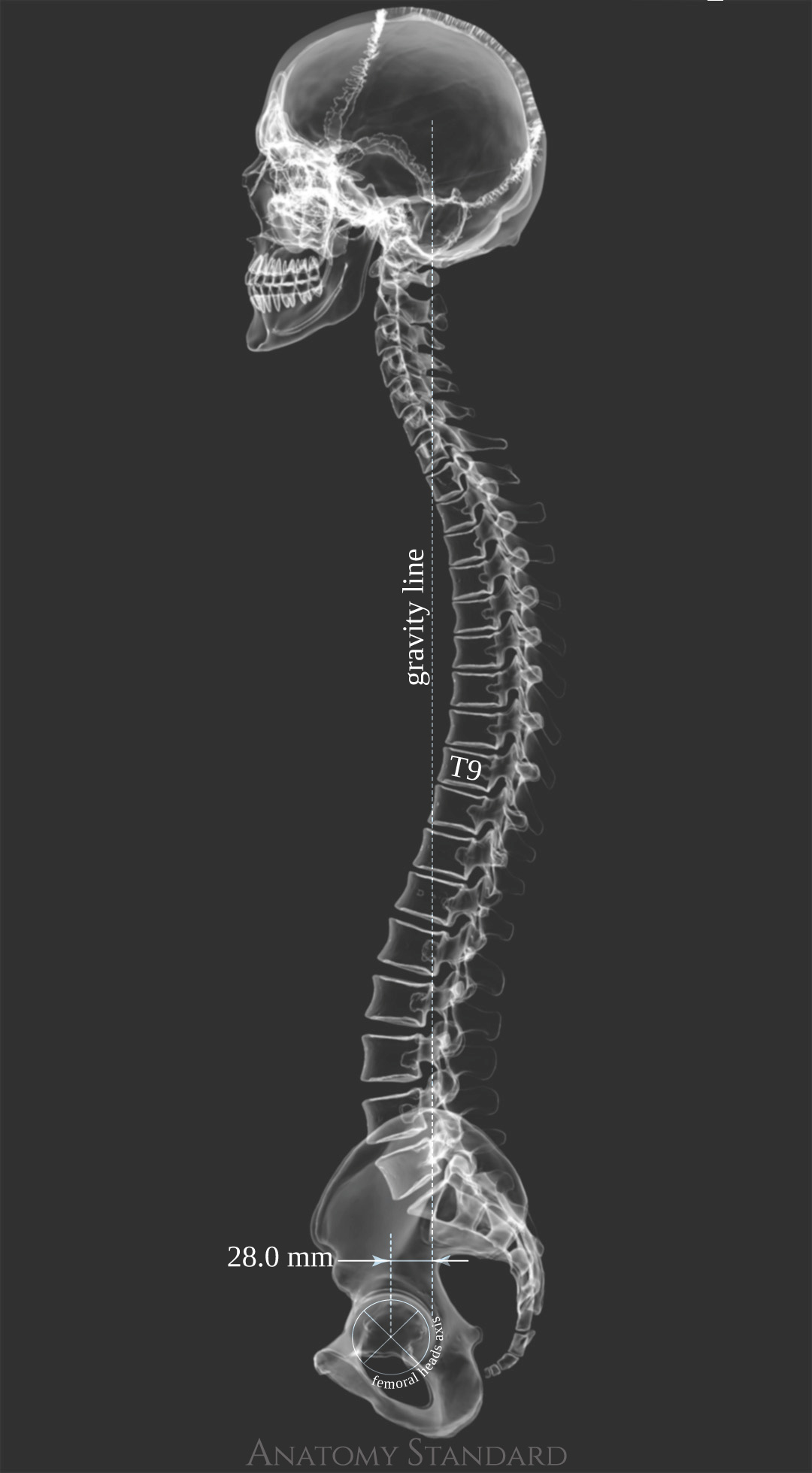

It was observed that the projection of gravity centers lies anteriorly at the thoracic levels and posteriorly at the lumbar levels, when the balance is optimal, as in healthy subjects (Legaye 2005).
List of references
Last update: Jan/2022